Purpose of the Guide
This guide is an overview of the United States Core Data for Interoperability (USCDI) and its application in digital quality measurement, particularly for HEDIS® reporting. It was designed for health care professionals, IT specialists and stakeholders in quality measurement and data interoperability, and offers practical steps and resources for utilizing USCDI.
Understanding USCDI

What Is USCDI?
USCDI is a standardized set of health data classes and constituent data elements that the health care ecosystem (e.g., clinicians, health information systems) uses to ensure consistent and accurate exchange of health information across systems and settings.
Who Developed USCDI?
USCDI was developed and adopted by the Assistant Secretary for Technology Policy (ASTP) on behalf of the U.S. Department of Health and Human Services (HHS). USCDI is incorporated into regulations from both ASTP and the Centers for Medicare & Medicaid Services (CMS), underscoring its significance in national health IT strategies.
Why Was USCDI Developed?
USCDI replaces the Common Clinical Data Set (CCDS) as part of ASTP’s efforts to enhance health data interoperability. It addresses the need for a standardized framework that supports consistent exchange of health information. Its aim is to enhance interoperability, improve care coordination, support health IT initiatives and ensure that health care practitioners, payers and partners can share critical patient information efficiently and accurately. The transition from CCDS to USCDI reflects expansion and refinement of the data elements required for health information exchange.
There are three guiding principles for USCDI:
- Define a core set of structured and unstructured data essential for supporting patient care and enabling patient access through health IT.
- Create a consistent foundation of harmonized data elements that can be applied across use cases, including those beyond direct patient care and access.
- Evolve through a predictable, transparent, collaborative approach, considering both the expected benefits and the broader impact on the health care industry.
What Is USCDI’s Relevance to Quality Programs?
USCDI supports quality measurement initiatives by providing a baseline-standardized dataset and associated vocabulary standards that facilitate accurate, consistent data exchange. For quality programs and health information exchange use cases, implementation of USCDI is supported by standards and guidelines, including FHIR® US Core profiles. Standardized data elements from USCDI are utilized in HEDIS digital measure specifications (via FHIR) to define clinical concepts, which helps ensure that quality measures are based on comparable and commonly defined data across health care practitioners and settings.
USCDI Versions
Each USCDI version builds on the previous one by adding new data elements and classes, and refining definitions or vocabulary standards based on stakeholder feedback. For example, USCDI v1 includes essential data classes like patient demographics and clinical notes, while subsequent versions expand to include additional elements such as social determinants of health (SDOH) and health status assessments.
Update Process
Creation of new USCDI versions is a structured, multi-step process managed by ASTP.
1. Call for Data Element Submissions
During the yearly submission period, stakeholders can propose new data elements or revisions to existing ones.
2. Review and Evaluation
New data elements are evaluated based on their relevance to patient care, feasibility of implementation and potential impact on improving health care interoperability and quality.
3. Release of Draft Version
After evaluation, ASTP releases a draft version of the new USCDI for public comment. This draft includes proposed new data elements and revisions to existing ones.
4. Public Comment
The draft version is available for public feedback, allowing stakeholders to express support, suggest changes or raise concerns about proposed updates. This period typically lasts several months.
5. Review and Revision
ASTP reviews the feedback and may revise the draft USCDI based on stakeholder input.
6. Publication of Final Version
ASTP publishes the final version of the updated USCDI on its website.
7. Ongoing Updates
This iterative process includes annual updates, allowing continuous improvement and adaptation of the USCDI to meet the changing needs of the health care landscape.
USCDI Updates Over Time
Annual USCDI updates reflect the evolving needs of health care interoperability. Updates incorporate new data elements and respond to stakeholder feedback, which may result in changes to existing elements. ASTP typically releases a draft version of USCDI in January, and a final version in July.
A view of USCDI updates over time shows the progression from USCDI v1 to the latest versions, highlighting the addition of new data classes and elements. This overview helps stakeholders understand the evolution and improvements made in each version.
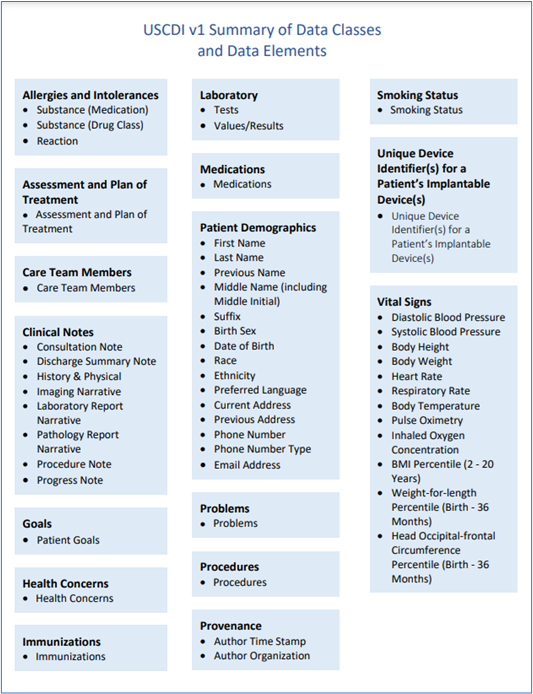
- USCDI v1 is required by Cures Act Final Rule; it comprises 16 data classes, including patient demographics, medications, laboratory, vital signs, clinical notes and provenance.
- USCDI v2 added 3 data classes and 22 data elements, including sexual orientation and gender identity (SOGI) and SDOH elements in support of advancing health equity.
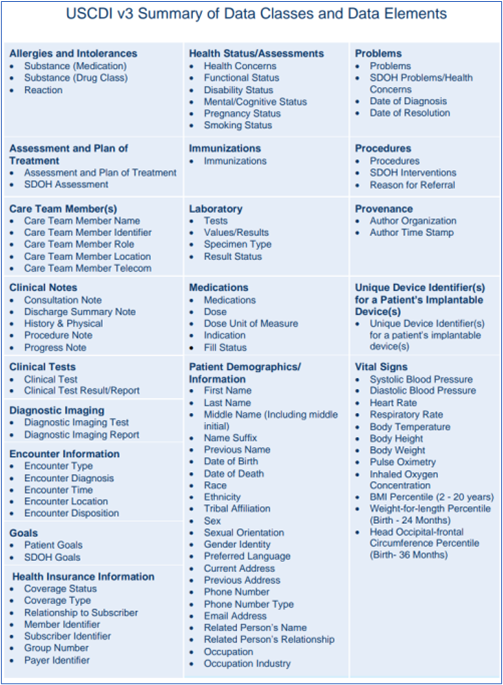
- USCDI v3 added 2 new data classes and 24 additional data elements focused on addressing equity, disparities and public health data interoperability.
- USCDI v4 and v5 continued to expand data classes and elements, but are not yet ASTP-required versions.
Summary of Data Classes and Data Elements USCDI v1 vs. USCDI v3
USCDI Version 1 is required under the Cures Act Final Rule. Certified health IT must support the data elements defined in USCDI v1 to facilitate standardized exchange of key health information.
USCDI Version 3 is expected to be required starting on January 1, 2026, per the HTI-1 Final Rule. Health IT vendors may voluntarily upgrade to newer versions not yet required by regulations, through the Standards Version Advancement Process (SVAP).
- https://www.healthit.gov/isp/sites/isp/files/2020-10/USCDI-Version-1-July-2020-Errata-Final_0.pdf
- https://www.healthit.gov/sites/default/files/facas/2022-08-17_USCDI_v3_Presentation_508.pdf
What’s the Standards Version Advancement Process (SVAP)?
The SVAP is a critical element of ASTP’s strategy to foster a more agile and responsive health IT environment, allowing continuous improvement in health care technology while maintaining compliance with federal standards. Under the SVAP, once ASTP approves a newer version of a standard or implementation specification, health IT developers can choose to integrate it into their certified systems before they are required to by federal regulations. This reduces lag time between release of a new standard and its adoption in the market, ensuring that health IT systems can quickly take advantage of improvements in data sharing and interoperability. This approach also accelerates availability of updated and more effective health IT solutions for clinicians and patients.
Key Components of USCDI
USCDI has two main parts, as defined by the ASTP:
- A data class—an aggregation of data elements by a common theme or use case.
- A data element—a portion of data defined in USCDI for access, exchange or use of electronic health information.
A data element in the USCDI typically includes specific information to guide its implementation and use in health IT systems. This information is often a definition, use notes or examples and, in some cases, associated vocabulary standards. These components ensure that the data element is understood and used consistently across systems, enhancing interoperability.
Data Class Examples
Patient Demographics/Information
Data used to categorize individuals for identification, record matching and other purposes. Includes essential information about the patient such as name, date of birth, race, ethnicity and gender identity. Accurate demographic data are crucial for patient identification and health equity.Procedures
Activities performed as part of care delivery. Include details about medical procedures performed and SDOH interventions.Laboratory
Analysis of clinical specimens to obtain information about a patient’s health. Includes the lab test and the value or result, which are vital for diagnosis and treatment planning.Medications
Pharmacologic agents used in diagnosis, cure, mitigation, treatment or prevention of disease. Information on medications, including drug names, dosages and fill status, supports medication safety and appropriate treatment.Clinical Notes
Narrative patient data relevant to the context identified by note types. Encompass progress notes, discharge summaries and relevant clinical documentation that provide a comprehensive view of the patient’s health status and care history.Health Status Assessments
Assessments of a health-related matter of interest, importance or worry to a patient, the patient's family or the patient's health care provider that could identify a need, problem or condition.Example of Data Elements
While data classes are related data elements, the elements themselves are the most granular level where data are exchanged, as shown in the example below.
| Data Class | Data Elements |
|---|---|
| Health Status Assessments Assessments of a health-related matter of interest, importance or worry to a patient, the patient's family or the patient's health care provider that could identify a need, problem or condition. |
|
About USCDI+
USCDI+ is designed to accommodate data needs that exceed standard USCDI. It allows inclusion of additional data elements or classes tailored to the unique requirements of federal agencies and stakeholders within the health care system, building on USCDI’s baseline set of data elements for nationwide interoperability. Some advantages of this approach are:
- Customization for Specific Needs. USCDI+ enables organizations—federal agencies, in particular—to define additional sets of standardized data elements that are critical to specific use cases. This ensures that data exchanged meet the precise needs of programs and initiatives for one use case while harmonizing and aligning across other use cases, where appropriate.
- Enhanced Interoperability. By expanding the standard USCDI to include specialized data elements, more comprehensive data exchange across health IT systems is enabled and standardized, leading to better coordination of care, improved public health reporting and more effective research outcomes.
- Flexibility and Scalability. USCDI+ provides a flexible framework that can be adapted as new data needs arise. This scalability allows continuous evolution of health IT systems to accommodate emerging priorities such as advances in medical research or public health surveillance.
- Alignment With Federal Priorities. USCDI+ supports federal health programs by aligning data exchange requirements with national health priorities, ensuring that data collected and shared are relevant to the goals of federal initiatives such as improving population health, advancing equity or enhancing health care quality.